Mast cell tumor (MCT) is the most common skin tumor found in dogs. While it can occur in a breed, Boxers, Boston Terriers, and Labrador Retrievers appear to have the highest incidence, with an average age of 9 years. Its etiology remains unknown, but chronic inflammation of the skin could be a predisposing factor. Although the genetic alterations that predispose some dogs to MCT are not fully understood, research has identified the expression of c-kit, a receptor tyrosine kinase. Several studies have shown the presence of mutations in c-kit, and based on this new information, new therapies are now available to treat MCTs.

What are mast cells?
Mast cells are cells that are normally found in all tissues of the body but mainly in the skin, respiratory tree and gastrointestinal tract and are part of the immune defense mechanism against invading microorganisms. Inside these cells are tiny granules that release different chemicals: mainly histamine (causes fluid leakage that leads to swelling and itching) and heparin (a blood anticoagulant) that targets invading parasites. We could liken it to “little bombs” that can explode and have an important role in allergic reactions, non-allergic skin diseases, wound healing and skin regeneration. In addition, they cannot cause increased secretion of gastric acids.

Mastocytomas are called Great Imitators – as they can look like anything! A cutaneous or subcutaneous mass is typically noted and is often an incidental finding and often misidentified as lipomas. The others are usually solitary, fixed nodules, but multiple lesions are seen in 5–15% of patients. Well- to moderately differentiated tumors tend to be solitary, slow-growing, and firm to variable in texture. Poorly differentiated tumors can have a more aggressive history, with rapid growth, possibly with intermittent tumor enlargement and pain. When they degranulate, due to the release of histamine, swelling and/or bruising of nearby tissues or even gastrointestinal symptoms may occur.
Diagnosis and clinical staging
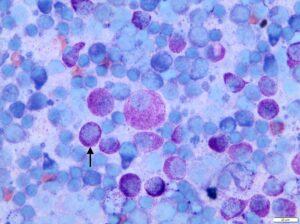
Diagnosis can often be made by fine needle aspiration (FNA), which collects some tumor cells with a needle and the cells are examined under a microscope. Granules have distinct staining characteristics that lead to their identification.
Recommended staging tests to be done before the tumor is removed include the standard pre-anesthetic blood test, fine needle aspiration (FNA) of the regional lymph node, chest x-rays and perhaps an abdominal ultrasound. Although MCTs rarely metastasize to the lungs, a chest X-ray will help rule out the presence of unrelated disease (or even a second tumor).
However, a tissue biopsy is required to stage the tumor to determine its prognosis.
GRADE I TUMORS
It is the mildest type of mastocytoma tumor. While it tends to be larger and more bifid locally than may be visually apparent, it tends not to spread beyond its location on the skin. Surgery should be curative. If the initial biopsy specimen shows that the tumor is only narrowly removed or that the tumor extends to the surgical margins of the specimen, a second surgery should be performed immediately to remove the remainder of the tumor, if possible. If the grade I mast cell tumor is not completely removed, it will recur at a later time. It is best to exclude it completely as soon as possible if its anatomical position allows. About half of mast cell tumors are Grade 1 tumors and can only be cured with surgery.
GRADE II TUMORS
This type of tumor is somewhat unpredictable in its behavior. Recent studies have shown that radiation therapy given to the site of the tumor can cure more than 80% of patients, as long as the tumor has not already shown metastatic spread.
GRADE III TUMORS
It is the most unfavorable type of mastocytoma there is. Grade III tumors account for approximately 25% of all mast cell tumors and behave very invasively and aggressively. If surgical resection alone is attempted without adjunctive chemotherapy, a median survival time of 18 weeks (4-5 months) can be expected.
A new 2-stage staging system (high grade versus low grade) is now proposed
SURGERY
Surgery is the treatment of choice for all MCTs unless the tumor is impossible to remove. If the tumor can be cured with one or even two surgeries, this is ideal. Mast cell tumors are highly invasive and require very deep and extensive margins (at least 3 cm in all directions, but it has been found that 2 cm margins may be sufficient for grade I and II tumors). This can be a problem for tumors located eg in the neck, mouth or other anatomical areas. In addition, the inflammation associated with handling the tumor can lead to additional swelling, bleeding, and even a drop in blood pressure. One study observed a 10% incidence of wound healing failure (“breakdown”) in mast cell tumors. The biopsy sample taken will not only determine the grade of the tumor but also include measurement of the normal tissue that has been removed around the tumor. The width of the margins will be very important in determining whether further treatment is needed. If the margins are tight or the margins indicate that there is still tumor, then a second surgery or even radiation therapy may be desirable. Clear margins are generally defined as a 10 mm margin around the tumor in all directions. If the margin is clean, theoretically the tumor has been completely removed, but it is recommended that the area be monitored over the next few years for any recurrence.

When should systemic treatment be done and what are the options?
Adjunctive therapy (chemotherapy, tyrosine kinase inhibitor [TKI] therapy) may be considered in dogs with poor prognostic markers (eg, grade III, high MI, difficult anatomic location, metastasis) after MCT resection. Dogs with unresectable tumors may also be considered for chemotherapy or TKI therapy. In general, chemotherapy is most successful against microscopic disease, but may be beneficial in cases with bulky tumors.





